Preguntas frecuentes
Implantes dentales
El proceso de oseointegración, se define como la unión mecánica firme, directa, estable y duradera producida entre el hueso vivo maxilar y el cuerpo de un implante dental de titanio, que acontece sin interposición de tejido conectivo.
Para que se produzca la oseointegración, hay que realizar una correcta técnica quirúrgica, dependiendo el éxito de la presencia o ausencia de procesos inflamatorios, del diseño del implante y del tiempo en el que el implante se mantenga libre de cargas, que debe ser alrededor de 4 a 6 meses.
En la actualidad, las técnicas más avanzadas como los implantes de carga inmediata permiten proporcionar una prótesis con dientes fijos sobre implantes oseointegrados a los pocos días o incluso a las horas de su colocación.
Existen muy pocas contraindicaciones absolutas, entre las que podemos destacar enfermedades graves que influyan en el metabolismo del hueso, infecciones específicas, tumores malignos que afecten al hueso, o radioterapia en grandes dosis.
Es importante decir que los implantes dentales no provocan rechazo en el organismo, comúnmente cuando se habla de rechazo se refiere a una no oseointegración del implante dental (se estima normal un nivel de fracasos del 2% a 5% de los implantes colocados). Cuando un implante dental no se oseointegra se puede volver a colocar otro para sustituirlo.
Se trata de una intervención ambulatoria, esto quiere decir que el paciente se trata en nuestra clínica dental.
La intervención se lleva a cabo en la mayoría de los casos mediante anestesia local. En intervenciones de larga duración (rehabilitaciones completas, elevaciones de seno maxilar, regeneración ósea) se puede recurrir a la sedación endovenosa realizada por un médico anestesista en la clínica dental.
Al contrario de lo que pueda parecer, en muchos casos el post-operatorio supone menos molestias e incomodidades que otras intervenciones menores en Odontología. Un implante a veces puede ocasionar molestias en la encía durante el proceso de cicatrización de la herida por lo que se prescriben analgésicos o antiinflamatorios según el tipo de intervención.
Es fundamental tener una buena higiene durante este periodo para evitar sobreinfecciones de la encía. Normalmente se prescriben antibióticos por seguridad. En los algunos casos aparece frecuentemente hinchazón durante los primeros días que suele remitir espontáneamente a las 72 horas, si bien no resulta dolorosa y permite hacer vida normal.
Las prótesis pueden colocarse tras tres a seis meses de espera una vez realizada la cirugía.
Los implantes se pueden colocar en los jóvenes una vez completado el desarrollo, normalmente a partir de los dieciséis años en las mujeres y dieciocho en los hombres. En los adultos no existe contraindicación en razón de la edad.
Básicamente existen dos formas de rehabilitación protésica sobre implantes: La prótesis fijas en zirconio o en metal-porcelana, que nos proporciona el mayor nivel de estética, comodidad y función, y la prótesis removible (de quitar y poner), realizada en resina y que supone una opción más económica al ser un tratamiento menos sofisticado, (sin dientes) y que necesitan más mantenimientos.
Para ello en clínica, el odontólogo toma impresiones y registros de mordida que posteriormente enviará al laboratorio donde el protésico vacía, o positiva, las impresiones en yeso, y confecciona sobre los modelos resultantes las estructuras de la prótesis fija con cera. Estos encerados se incluirán en revestimientos especiales resistentes a altas temperaturas, y se procede al colado en metal con distintas aleaciones.
El último paso podría ser montar la cerámica sobre las estructuras metálicas, dependiendo del tipo de prótesis fija a realizar, ya que también existe la posibilidad de realizar las coronas y puentes en porcelana pura (sin metal) o sobre una base de un material blanco llamado alúmina o zirconio que en este último caso se utiliza la innovadora tecnología de cadcam.
Los implantes correctamente colocados garantizan unos resultados estéticos en la mayoría de los casos muy superiores a la dentadura original del paciente.
El paciente debe tener claro que no sólo conseguirá una boca sana sino además una sonrisa estética. Esas deben ser sus exigencias.
Unos implantes bien colocados y de tamaño proporcional a la carga que han de soportar (a mayor tamaño mayor seguridad) son para toda la vida.
Las condiciones fundamentales para garantizar el éxito son:
1.La correcta planificación del caso concreto
2. Las manos y la experiencia del cirujano (el tamaño del implante y su correcta colocación)
3. La elaboración de la prótesis teniendo en cuenta las cargas que ha de soportar y el correcto ajuste para evitar fuerzas anómalas que supongan un sobreesfuerzo de los implantes
Quizás el riesgo más significativo es la pérdida de sensibilidad en la zona del labio inferior cuando durante la intervención se toca o se secciona el nervio mentoniano, dicha pérdida de sensibilidad puede ser temporal o permanente.
Por ese motivo hay que ser especialmente cuidadoso cuando se opera en esa zona porque no nos vale tocar el nervio con un implante demasiado largo pero tampoco nos sirve un implante demasiado corto que no aguante la carga a la que será sometido.
Por otro lado es fundamental que los implantes estén correctamente colocados desde un principio, puesto que una vez que éstos se oseintegran quedan “soldados” al hueso y si fuese necesario extraerlos perderíamos mucho hueso maxilar, lo cual complicaría enormemente una rehabilitación y por supuesto los resultados nunca serían los mismos.
Hoy en día disponemos de técnicas avanzadas para realizar cirugías en casos extremos. Se puede recurrir a elevaciones de seno maxilar e injertos que pueden ser autólogos (propios del paciente) o de otros tipos, con un porcentaje de éxitos elevadísimo.
Afortunadamente son rarísimos los casos en los que un paciente que desea ser rehabilitado no puede serlo. El campo de la regeneración ósea es sin lugar a dudas uno de los principales avances en la implantología de los últimos años.
Para los pacientes con piorrea los implantes son “LA SOLUCIÓN”. Tradicionalmente este tipo de pacientes estaban ineludiblemente abocados a perder sus dientes.
El único tratamiento que podíamos ofrecerles era una higiene escrupulosa y periódicas visitas a la consulta para realizarse tratamientos periodontales. La perspectiva final siempre era la misma: la dentadura completa de quitar y poner.
Ahora los implantes han revolucionado la forma de tratar a estos pacientes, es importantísimo saber que los largos tratamientos periodontales no solo son inútiles sino que son perjudiciales porque mientras se hace un esfuerzo para conservar la pieza natural no podemos evitar que la enfermedad siga su curso y vayamos perdiendo hueso. Hay que saber cortar ese proceso antes de que sea demasiado tarde.
El hueso es fundamental para una buena rehabilitación y para un resultado estético. En los casos extremos es muy difícil lograr estética.
Quizás sea el único caso en la medicina en el que el sustituto artificial tiene una mejor funcionalidad que el órgano original.
Un implante que trabaja correctamente en la boca (porque está colocado en la posición idónea y soporta una carga axial y proporcional a su tamaño), tiene una durabilidad muy superior a la vida natural de un diente.
Al Hablar de implantes sin cirugía estamos hablando de procedimientos de cirugía a ciegas guiada por ordenador. Todos estos sistemas utilizan una plantilla elaborada previamente sobre la cual hay que adaptar los implantes y que nos permite colocarlos sin tener que abrir la encía ni dar puntos.
Lógicamente la intervención es menos invasiva, pero una mínima variación en la posición en boca de la plantilla podría dar problemas.
Solamente es recomendable hacerlo en casos muy concretos y favorables. Aún así la calidad de la prótesis que se puede ofrecer en estos casos está muy condicionada por el factor tiempo. En estos casos nosotros ofrecemos dientes provisionales en resina que luego serán sustituidos por los definitivos en cerámica de máxima estética.
Los tratamientos en cerámica no pueden realizarse en el día, solamente es posible hacer prótesis de resina prediseñada, por lo tanto no personalizada.
Aquellos que hemos comentado en la pregunta anterior, en los que la prótesis se coloca el mismo día de la cirugía.
El zirconio es un excelente material en el campo dental, tiene una máxima biocompatibilidad (la misma que el titanio) y permite realizar prótesis de una estética insuperable. Sin embargo su uso en el ámbito quirúrgico en odontología es reciente y muy minoritario.
Se puede decir que como implante, es decir dentro del hueso, no aporta ninguna ventaja añadida con respecto al titanio. Es una opción del profesional.
Preguntas frecuentes
Ortodoncia
To correct a bad correspondence between the lower and upper dental arch and/or an anomalous alignment of the teeth.
The most frequent cases that require orthodontic treatment are:
– Overcrowded or overlapping teeth
– Overbites or underbites
– Open bites (posterior teeth close but not the front teeth)
– Too much or too little space between teeth
– Extra or missing teeth
It is a technique that is increasingly used, given the current interest in promoting the health of our children.
It is increasingly requested at younger ages.
The forces applied to move the teeth are very gentle, so after the first few days you will not notice anything special.
Yes, totally.
Orthodontic appliances will not interfere with your usual activities.
Some recommendations should be followed when eating or brushing your teeth.
They will not change the way you speak, and you can maintain your professional activity and social relationships without any interference.
All treatments require proper maintenance. With the help of fixed lingual retainers or removable retainers, the results obtained can be stable, being an investment for life.
They can be caused by:
– Bad habits (thumb sucking, swallowing with interposition of the tongue, etc.).
– Mouth breathing (due to adenoid hypertrophy -vegetations-, etc.).
– Ectopic dental eruption (a tooth located in a different place than its natural location).
– Dental agenesis (the lack of one or more teeth).
– Supernumerary tooth (larger number of teeth than usual).
– Skeletal craniofacial skeletal dysplasias (congenital alterations of the bones of the face and head).
– Space problems (occurs when the maxillary bone is still infantile and the teeth are definitive, which are larger and in greater number).
It is used in children and adolescents because they are in the midst of skeletal growth and tooth replacement, and can therefore act on both structures.
Once growth is complete, only the teeth can be treated. In women, the end of craniofacial growth is considered to be at the age of fifteen and in men at the age of nineteen.
Although it can be used at any age, orthodontics is capable of correcting the bad position of the teeth to achieve a healthy mouth. A beautiful smile brightens the face and makes them more attractive.
The bone of the jaws, although very hard, is also very flexible.
The biological process involved in tooth movement is the same at any age, so teeth can move at age 20 as well as at age 60.
It is not only a matter of coquetry, it is also a matter of health. A bad position of the teeth can favor the appearance of other problems such as caries, periodontal (gum) disease or joint problems.
The spectacular aesthetic improvement of fixed orthodontic appliances (brackets) allows adults of any age who are dissatisfied with the appearance and/or function of their mouth (crowded teeth, spaces between teeth, protruding teeth, etc.) to stop feeling limited and accept orthodontics as normal.
Ceramic brackets, which resemble tooth enamel and have no visible metal, go almost unnoticed by others and satisfy most adults.
It is difficult to establish at what age a child needs orthodontic treatment.
If we take into account that children between 7 and 12 years of age are in the period of changing teeth (exfoliate temporary or milk teeth for the arrival of the permanent or definitive teeth), a clinical and radiographic evaluation is recommended around the age of 7 years to begin to observe and control the correct dentofacial growth during this period.
Sometimes, when there are obvious problems, it may be advisable to visit children before the age of 7 in order to provide early treatment.
Thus, in some patients we will intervene early – early treatment – often obtaining unattainable results only with orthodontics once skeletal growth is complete, while in others, even if the problem is evident, we will recommend waiting, periodically checking the children while the teeth erupt and the facial bones develop.
In adults, treatment can be initiated at any age.
It is difficult to evaluate exactly the problems in the future, but normally the alterations will surely worsen with the passage of time, especially in a child or adolescent, we must not forget that it is in development and the dento-facial problems will also grow.
It is convenient to treat it for two fundamental aspects:
– If the anomaly is detected and treated in time, it will be treated more easily, reducing discomfort, time and cost.
– We could avoid a more complex bone treatment (maxillofacial), avoiding possible anomalies in the bones, which would be reflected in the appearance of the face.

Preguntas frecuentes
Carillas dentales

To correct a bad correspondence between the lower and upper dental arch and/or an anomalous alignment of the teeth.
The most frequent cases that require orthodontic treatment are:
– Overcrowded or overlapping teeth
– Overbites or underbites
– Open bites (posterior teeth close but not the front teeth)
– Too much or too little space between teeth
– Extra or missing teeth
It is a technique that is increasingly used, given the current interest in promoting the health of our children.
It is increasingly requested at younger ages.
The smile is one of the most important aesthetic factors inherent to the person. A beautiful and attractive smile offers a positive image and stimulates the individual to smile calmly and naturally.
A tidy, healthy and harmonious mouth gives self-confidence.
Preguntas frecuentes
Coronas de zirconio
La Estética Dental, como su nombre lo sugiere, cubre todo aquello que tenga que ver con la belleza, la estética, o el embellecimiento de sus dientes, en sus muy distintas formas y posibilidades.
Es la rama de la odontología que va a tratar todas aquellas alteraciones y patologías de la morfología bucodental para alcanzar un canon de belleza ideal.
En la actualidad tener una buena sonrisa es un claro ejemplo de salud y bienestar social.
Causas por las cuales los pacientes pueden acudir a estos tratamientos:
1. Asimetrías dentarias (dientes apiñados o desparejos)
2. Diastemas interincisivos (separación entre dientes anteriores)
3. Cambios de coloración o dientes pigmentados o manchados
4. Caries de cuello
5. Fracturas dentarias
La sonrisa es uno de los factores estéticos más importantes, inherentes a la persona. Una sonrisa bonita y atractiva ofrece una imagen positiva y estimula al individuo a sonreír con tranquilidad y naturalidad.
Una boca ordenada, sana y armónica da seguridad en uno mismo.
Indicaciones. Se emplean cuando se ha perdido una gran cantidad de tejido dentario, por ejemplo tras una gran caries o un traumatismo, ya que la retención de una carilla o un empaste resultaría muy difícil debido a la gran pérdida de tejido dentario.
También se emplean en casos de dientes endodonciados, para dar consistencia a todo el diente y evitar posibles fracturas, ya que los dientes endodonciados se debilitan con el paso del tiempo.
Contraindicaciones. Prácticamente cualquier paciente puede llevar coronas, a excepción de aquellos que:
1. Presenten problemas de encías en estado avanzado
2. Que el diente tenga algún problema que limite su conservación en la boca
3.Tengan excesiva movilidad dental
Las coronas están confeccionadas de un material tan resistente que a veces pueden durar incluso más de 50 años. No obstante, debido al desgaste natural que produce la masticación, a veces pierden la forma o el brillo. En estos casos y si el paciente lo desea, se extrae la corona y se vuelve a colocar una nueva.
Preguntas frecuentes
Periodoncia
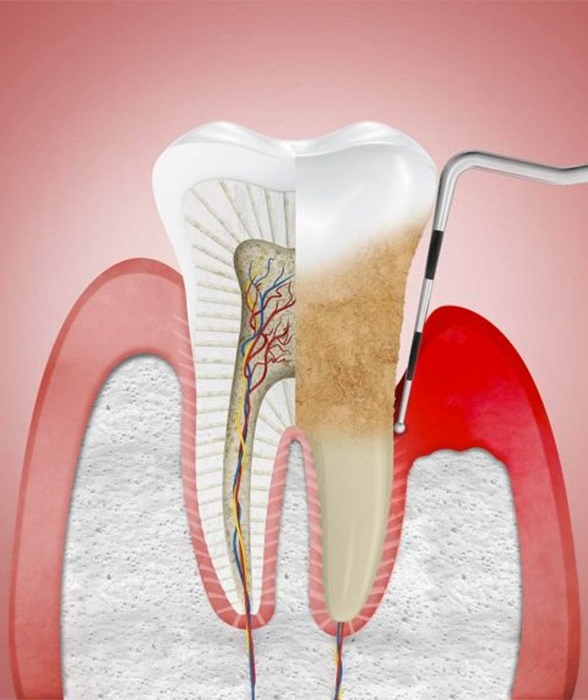
Periodontal diseases are a group of diseases that affect the tissues (periodontium) that surround and support the teeth in the jaws.
They are diseases of an inflammatory nature and of infectious cause (caused by bacteria) that depending on their degree of affectation are called gingivitis, when the inflammatory process only affects the superficial periodontium (the gum) and the tissues that support the teeth are not affected.
When the inflammatory process affects the deep periodontal tissues, there is destruction of the bone and periodontal ligament, which are the tissues that support and hold the teeth. This degree of involvement is called periodontitis.
There are several stages of periodontitis from the early stages to the most advanced. If periodontitis is not treated it evolves destroying all the support of the tooth and with it the lodging and loss of the tooth. For this reason it is important to detect periodontitis and treat it in its earliest stages.
Gingivitis, in addition to producing gum inflammation and bleeding, especially when brushing, in some individuals evolves into periodontitis. Periodontitis, when the bone that supports the teeth in the jaws is destroyed, causes mobility and separation of the teeth.
Eventually the teeth will end up being lost, either because of the need to extract them due to their instability or because they fall out practically on their own.
It is due to bacteria that we all have in the mouth, around the teeth, and if we do not eliminate them correctly, they gain access to the space between the tooth and the gum and can colonize this space growing in number and causing the inflammatory and destructive reaction that defines these diseases.
Bacteria by themselves are not capable of causing the consequences of these diseases, but need a susceptible individual (genetic predisposition) and a suitable environment (factors such as tobacco and stress are very important risk factors in the colonization of these bacteria).
Gingivitis is one of the most common diseases in humans, very frequent in all age groups (in young people 75% between 20 and 25 years of age).
Some gingivitis, even in the absence of treatment, does not progress to the destruction of the periodontal tissues supporting the teeth (periodontitis).
Periodontitis is very rare in young people and adolescents (approximately 1 case/10,000). However, its frequency increases with age. It affects approximately 80% of the adult population over 35 years of age.
Therefore, it is a relatively frequent disease in adults and its frequency clearly increases with age.
In the initial stages it can be corrected. But it tends to be a chronic condition. This means that when the stage of the disease is advanced and much bone support has been lost, the most that can be done is to stop the progression of the disease so that it does not go further.
The patient should be aware of his problem and assume that, after the initial treatment, at least once a year should go to the dentist for maintenance cleanings, for the rest of his life. Oral hygiene is fundamental to treat this type of problem. This is the only way to achieve an effective therapy.
The basic treatment consists of a thorough cleaning of the gums by means of an ultrasonic device, curettes (sweeping instruments) and polishers. All this is aimed at eliminating all the bacterial plaque causing the problem. The patient is able to clean the part of the teeth exposed in the mouth, but cannot access the part of the tooth below the gum. This is the task to be performed by the dentist, so that after cleaning, the inflation decreases and the gum reattaches to the tooth forming a barrier to prevent bacteria from passing through.
The basic treatment is performed in parts. The mouth is divided into 4 quadrants, each of which is treated in different sessions. Each cleaning session is performed under local anesthesia, so it does not hurt. Its duration is about 45-60 min. At the end of the session and after the anesthetic effect subsides, the patient reports very little discomfort, and in 3 or 4 days the state of the gums improves amazingly. From this moment on, it will be the patient who must maintain the health of his gums and attend periodic check-ups every 4 or 6 months.
Regenerative treatment, in severe cases, when the affectation is very pronounced and has been prolonged in time, the patient has experienced a considerable loss of bone. In these cases, before any restorative treatment, it is necessary to replace the lost structures as far as possible. For this purpose, various biomaterials are used: membranes, amelogenin, bone, etc.
All of these are effectively combined to restore the lost anatomy.
Fighting dental plaque and preventing tooth and gum disease.
1. Dental Floss: Use dental floss to remove germs and food particles between the teeth. Rinse.
How to hold the floss.
To remove plaque between the upper teeth use the floss by moving it up and down.
To remove plaque between the lower teeth use the floss by moving it up and down.
*Note! Insert the floss between the teeth gently. Do not “snap” it in, this could hurt the gums.
2. Toothbrush: Use whatever method of brushing your teeth is most comfortable for you, but don’t scrub them vigorously back and forth. Small circular motions and short back and forth strokes are best. Rinse.
To prevent cavities, what you put on your toothbrush is important.
Use a fluoride toothpaste.
Fluoride protects teeth against cavities.
Preguntas frecuentes
Odontopediatría

The main difference between normal dentistry and pediatric dentistry in the treatment of caries is the presence of primary or baby teeth in children, which changes the treatment, so that lesions occurring in the primary dentition will be treated in a less conservative and more aggressive manner than those occurring in the permanent teeth, to avoid that, in the worst case scenario, an insufficient treatment could be given to a primary tooth that would then have repercussions on its successor, the permanent tooth.
Sealants to stop caries: These are resins that are applied on the chewing surfaces of the teeth. They reduce the probability of caries in the teeth on which they are placed. They act as protective barriers, preventing food debris from lodging in the reliefs of the teeth.
They turn the chewing surfaces of the teeth into smooth surfaces that are easy to clean. They are usually applied in children from 6 to 7 years of age, when the permanent teeth begin to erupt.
Although the sealant facilitates cleaning, brushing should not be neglected, if proper hygiene is not carried out, a cavity may appear near the sealant. The placement of sealants does not damage the enamel, does not require anesthesia, the dentist brushes the piece and brushes it with a cream, which hardens when a special light is applied. Sealants last for a long time, but it is necessary a periodic control by the dentist to check their condition.
Cavity bases and linings: For the base or bottom of the cavity calcium hydroxide, zinc oxide eugenol is used, which is an antibacterial substance that forms secondary dentin, glass ionomer that releases fluoride and, previously, polycarboxylate cement and zinc phosphate were used, but they are no longer used because they are very toxic.
Temporary materials: These are materials used for a limited time until permanent material is available.
Definitive materials: these are the materials that we will use in the definitive fillings.
Silver amalgam: The only one we can use in unsuitable conditions such as a difficult tooth or difficulty to isolate it.
Fluoride: It takes care of our enamel.